
Need a little clarity on COVID-19? I’ve been listening, watching, and paying attention daily. Assessing COVID-19 and its impact has been difficult in my opinion due to the sporadic testing data and the lack of confidence from information coming out from other counts.
I’ve got a few opinions based upon the best facts I can find. My first point is the reason I started this article.
POINT 1:
When assessing COVID-19, the article gives me the best picture of a true death rate that I have yet to see. This also demonstrates how valuable antibody testing can be to determine the true infection rate of an area.
The WHO reported a death rate of 3.4% a while back and common sense told me that 10 million people were not going to die in the United States from COVID-19.
A survey in New York State (they did 7,500 people, which is a significant number): 14.9% of the population have antibodies (essentially meaning that they were likely infected with this specific strain of coronavirus).
The state population is approximately 20 million
~15% of 20 million is 3 million
Approximately 3 million have been infected with COVID-19
Total deaths: 22,000
22,000/3,000,000 = 0.007
or 0.7% death rate
The reported influenza death rate is 0.1% (which varies from year to year)
I do consider this very serious and according to these numbers is 7x more lethal than influenza. It is NOT 34x as lethal as influenza as determined by WHO a while back.
POINT #2
I consider this statement from WHO TOTALLY MISLEADING: From an article in The Hill – “WHO says there’s ‘no evidence’ recovered coronavirus patients won’t get reinfected”
In a world filled with fear and panic right now, I think this statement is irresponsible.
Other than anecdotal reports of likely lingering COVID-19 infections being considered “reinfections”, the idea that you won’t have protection against this current COVID-19 strain would go against everything we know about immunology.
Unless there is a dramatic change in the virus, if you get infected I’d bet everything I own that you will not get reinfected. In the odd chance you would test positive, your symptoms would be minimal or non-existent if your immune system is functioning normally.
https://thehill.com/…/494628-who-says-theres-no-evidence-re…
POINT #3
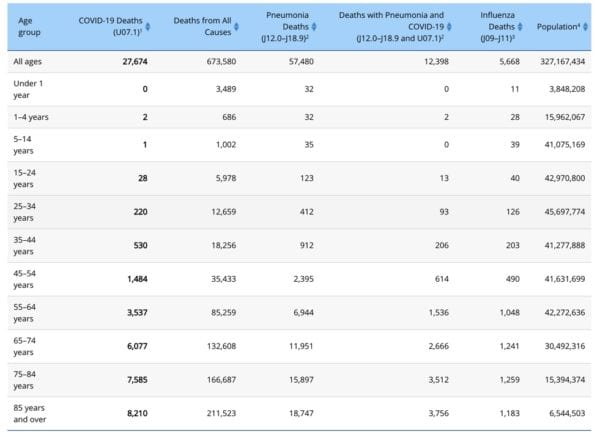
I’m encouraged that children seem to virtually not be affected. I’ve attached a table and there are way fewer deaths in kids versus influenza. They are likely to transmit the infection. I think the overall data lends towards continued common sense social distancing to slow the spread and ensure our healthcare facilities are not overwhelmed, with stay at home recommendations for people over 60-70 years old and those with high-risk conditions.
My biggest concern is for the elderly and immunocompromised where death rates are going to be significantly higher than 0.7%.
POINT #4
I believe that infection rates will slow in the summer and pick back up whenever we reopen schools. There will be cases in the summer, but I don’t believe there will be major outbreaks like we saw in NYC. There was some recent science on this that backs up the idea of this being a fall/spring/winter disease much like influenza: https://www.health.com/…/does-sunlight-really-kill-covid-19…
POINT #5
If you work in a factory, office, or another area where you see a lot of people or are in relatively close contact, you greatly increase your chances of getting infected. You can see the outbreaks going through various businesses that rely on large numbers of workers in a confined area.
When things open up, if you can work from home, I would do that as much as you realistically can.
The same goes for urban versus rural areas. Urban areas where there are more common areas and shared spaces (such as public transportation) are going to be hit harder and faster than rural areas. Again with the exception of close living areas in rural areas such as apartments, LTC facilities, etc.
POINT #6
Any articles based off of China’s data should be considered toilet paper and be treated as such. It might help the current shortage.
POINT #7
My optimism for a “cure” in the next 6 months is low. The original hydroxychloroquine article had more holes in it than swiss cheese. Vaccination will get us out of this, but we may reach herd immunity through natural infection before that happens. I hope I am wrong.
POINT #8
Thank you to all my healthcare friends that have sacrificed their health, well-being, and financial stability in all of this chaos.
Feel free to comment/critique my math and assumptions as there are various arguments to be made.
- 30 medication mistakes PDF
- 18+ Page Drug Interaction PDF
- 10 Commandments of Polypharmacy Webinar based on my experiences in clinical practice


Thank you for this insightful summary!
Great article. But for your point 2, I had the same opinion as yours until a few days ago. I’ve been digging deeper into immunology recently while reading about COVID-19, and learnt something called “antibody dependent enhancement”. [https://en.wikipedia.org/wiki/Antibody-dependent_enhancement]
Gosh, I have to say immunology is the most complicated subject I’ve ever come across.
This was great, thank you. I am working behind the counter in a community pharmacy and the panic all around me leaves me with little energy at the end of these endless days. This article gave me just enough of what I needed to know without the sensationalism, fear-mongering or ignorance that seems to spread as fast as this virus.
Good read!
Thanks for this blog, Ed.
Maybe the COVID19 ressource center of the European Hospital Pharmacists’ Association contains information that is of interest also outside Europe. Happy to share: https://www.eahp.eu/hp-practice/hospital-pharmacy/eahp-covid-19-resource-centre
By the way, the definitions of a SARS-CoV1 infection, COVID-19 disease and COVID-19 deaths are so heterogeneous across countries and have changed so frequently even within countries that it is impossible to compare mortality rates between countries or between past and present. Enumerator and denominator of that equation are just too different. As is the testing frequency and strategy across the world that adds to the varibility.
Stay safe!
Point no 7, herd immunity by natural infection is the possible remedy, good point. Does it by natural , fine. If not …say artificial. Viral load will define the fate.
Good statistics and well said. Herd immunity is defined by the viral load.
What is the situation with Ivermectin, Doxycycline & Zinc as opposed to Hydroxychloroquine?
Hi George, we recently did a recent post on a couple of these drugs – https://www.meded101.com/ivermectin-and-hydroxychloroquine-covid-treatments-or-not/